praegune kellaaeg 11.08.2026 20:36:06
praegune kellaaeg 11.08.2026 20:36:06 |
|
Hinnavaatlus
:: Foorum
:: Uudised
:: Ärifoorumid
:: HV F1 ennustusvõistlus
:: Pangalink
:: Telekavad
:: HV toote otsing
|
|
| Mitu last sul on? |
|---|
| 1 |
|
27% |
[ 11 ] |
| 2 |
|
30% |
[ 12 ] |
| 3 |
|
10% |
[ 4 ] |
| 4 |
|
7% |
[ 3 ] |
| 5 ja rohkem |
|
2% |
[ 1 ] |
| Ei ole ühtegi ja ei plaani ka teha |
|
20% |
[ 8 ] |
| Ei ole veel ühtegi, aga plaanin tulevikus teha |
|
2% |
[ 1 ] |
|
| hääli kokku : 40 |
|
| autor |
|
Tanel
HV Guru

liitunud: 01.10.2001
 
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
   |
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
 |
Hiid
HV Guru

liitunud: 23.03.2002
|
 23.04.2026 21:21:27
23.04.2026 21:21:27
|

|
|
| Tanel kirjutas: |
commer, lisasin küsitluse  |
algus on ehmatav  
_________________
Hapud viinamarjad |
|
| Kommentaarid: 664 loe/lisa |
Kasutajad arvavad: |
|
:: |
3 :: |
0 :: |
512 |
|
| tagasi üles |
|
|
degrass
HV kasutaja

liitunud: 23.12.2004
|
|
23.04.2026 23:16:48
|
|
|
Summary
The number of children in Western societies is influenced by various factors such as economic conditions, education levels, housing costs, substance use, and government policies. Key findings include:
- Negative factors affecting fertility:
-- Women's education and labor force participation
-- Economic uncertainty and unemployment
-- High housing costs delaying family formation
-- Delayed childbearing and obesity
-- Lack of supportive family policies and individualism
- Positive factors influencing fertility:
-- Low-cost childcare, paid parental leave, and paternal involvement in childcare
-- Higher household income and religiosity
- Political orientation and number of children:
-- Conservative/right-leaning individuals tend to have more children than liberal/left-leaning counterparts.
- Household income and number of children:
-- Complex relationship with higher-income areas having lower birth rates at the population level, but individual-level factors like sex and income type also play a role.
- Economic crises and fertility:
-- Recessions and economic downturns cause delays in childbearing due to job loss or financial instability.
-- The COVID-19 pandemic affected birth rates differently depending on country-specific contexts and policy responses.
- Housing costs:
-- High housing costs significantly influence age at first birth, delaying family formation among young adults.
- Substance use and fertility:
-- Tobacco smoking reduces female fertility by affecting ovulation and increasing miscarriage risk.
-- Alcohol consumption affects female fecundability in a dose-dependent manner.
-- Cannabis use may reduce sperm count in men and interfere with reproductive processes.
- Parental influence on offspring's reproductive behavior:
-- Low parental socioeconomic status predicts early childbearing in daughters, while higher parental education and income may delay childbearing but increase the likelihood of having more children later on.
-- Intergenerational transmission of family size is evident, with parents' family environment shaping their children's reproductive decisions.
- Government family policies:
-- Subsidized childcare, paid parental leave, and cash benefits have modest but positive effects on fertility rates.
-- No single policy is universally effective in isolation; a comprehensive approach is necessary to address the complex factors influencing family planning.
In conclusion, family planning and the number of children are shaped by a complex interplay of economic, social, educational, and policy-related factors that collectively influence fertility decisions across generations. Understanding these factors can inform policies aimed at supporting families and promoting healthy reproductive outcomes.
PS! pikk lugemine, Markdown
 Spoiler Spoiler
| tsitaat: |
## Main Factors Influencing Family Planning and Number of Children in Western Societies
**Negative factors** (associated with lower fertility) include **women's education and labor force participation, economic uncertainty, unemployment, housing costs, delayed childbearing, obesity, lack of supportive family policies, and value shifts toward individualism**. **Positive factors** (associated with higher fertility) include **free or low-cost childcare, paid parental leave, paternal involvement in childcare, higher household income, and religiosity**.[1][2][3]
### Negative Factors Reducing Fertility
**Socioeconomic barriers** represent the most significant constraints on fertility in Western societies. Lower educational attainment and lower household income are associated with reduced fecundability (probability of conception per menstrual cycle).[4][5] A Danish preconception cohort of 10,475 women found that compared to those with the highest education level, fecundability was substantially lower for women with primary/secondary education (FR: 0.73), vocational education (FR: 0.81), and lower tertiary education (FR: 0.87).[5] Similarly, household income below 25,000 DKK monthly was associated with 22% lower fecundability compared to incomes above 65,000 DKK.[5]

Figure 1
Associations of Poverty, Educational Level of Women and Men, and Household Income With Fecundability
undefined
**Economic uncertainty and unemployment** have consistent negative effects on fertility rates. A multinational analysis of 30 OECD countries from 1976-2014 revealed that increases in unemployment significantly reduced fertility rates in both Western European (−0.00256; p [6]
**Postponement of childbearing** is driven by multiple factors including women's increased education and labor market participation, effective contraception availability, value changes emphasizing self-fulfillment over procreation, partnership instability, housing costs, and absence of supportive policies.[1][7][8] This delay creates a fundamental conflict between the optimal biological period for reproduction and the time needed to complete education and establish careers.[1]
**Lifestyle and environmental factors** also contribute to declining fertility. Obesity negatively affects fertility rates in Western European countries.[6] Environmental exposures to chemicals from fossil fuels, including endocrine disruptors, may be contributing to deteriorating reproductive health, though causality remains under investigation.[9] Additionally, inadequate knowledge of female reproductive aging, particularly among men, contributes to delayed childbearing and subsequent fertility challenges.[2]
### Positive Factors Supporting Higher Fertility
**Family-supportive policies** can effectively counter fertility decline. Countries with improved provision of free or low-cost childcare, paid parental leave, and higher paternal contributions to childcare have seen increases in total fertility rates despite continuing trends toward older age at first birth.[2] Sweden increased its total fertility rate from 1.5 in the late 1990s to 1.9 in 2019 through such policies, though similar approaches had limited success in Singapore and Taiwan.[10]
**Higher socioeconomic status** shows complex relationships with fertility. While globally education correlates negatively with fertility, Western Europe shows a unique pattern where total fertility rate actually increases with education and decreases with religiosity.[3] At the individual level, higher household income is associated with better fecundability.[5]
**Religiosity** positively correlates with fertility rates across most global regions, potentially counteracting ongoing fertility decline in some areas.[3]
### Key Studies
Mills et al. (2011) conducted a systematic PRISMA review examining reasons for birth postponement and social policy effectiveness, identifying central drivers including contraception, women's education and employment, value changes, gender equity, partnership changes, housing conditions, and economic uncertainty.[1]
Götmark and Andersson (2020) analyzed 141 countries across six global regions, finding that fertility correlates negatively with education, contraceptive prevalence, and GDP per capita, while correlating positively with religiosity. Notably, Western Europe showed unique patterns where fertility increased with education.[3]
Jørgensen et al. (2023) followed 10,475 Danish women in a preconception cohort, demonstrating that both lower educational attainment and lower household income were independently associated with reduced fecundability, with effects persisting after adjustment for confounders.[5]
Anderson and Hickey (2023) reviewed demographic transitions in high-income countries, noting that while total fertility rates remain below replacement levels, some countries with greater prosperity and supportive policies are experiencing modest increases despite older maternal age.[2]
Aitken and Norman (2025) examined the interplay of social, environmental, and genetic forces, arguing that prolonged subreplacement fertility may permanently compromise human fecundity through reduced evolutionary selection pressure, increased reliance on assisted reproductive technology, and environmental pollutant exposure.[7]
## References
1. Why Do People Postpone Parenthood? Reasons and Social Policy Incentives. Mills M, Rindfuss RR, McDonald P, te Velde E. Human Reproduction Update. 2011 Nov-Dec;17(6):848-60. doi:10.1093/humupd/dmr026.
2. Reproduction in a Changing World. Anderson RA, Hickey M. Fertility and Sterility. 2023;120(3 Pt 1):415-420. doi:10.1016/j.fertnstert.2022.12.013.
3. Human Fertility in Relation to Education, Economy, Religion, Contraception, and Family Planning Programs. Götmark F, Andersson M. BMC Public Health. 2020;20(1):265. doi:10.1186/s12889-020-8331-7.
4. Poverty and Social Disadvantage in Women and Men and Fertility Outcomes. Boxem AJ, Mulders AGMGJ, van Rossum I, et al. JAMA Network Open. 2025;8(9):e2532741. doi:10.1001/jamanetworkopen.2025.32741.
5. Socioeconomic Status and Fecundability in a Danish Preconception Cohort. Jørgensen MD, Mikkelsen EM, Hatch EE, et al. Human Reproduction (Oxford, England). 2023;38(6):1183-1193. doi:10.1093/humrep/dead077.
6. Influence of Obesity and Unemployment on Fertility Rates: A Multinational Analysis of 30 Countries From 1976 to 2014. König-Castillo DM, Ott J, König D, et al. Journal of Clinical Medicine. 2022;11(5):1152. doi:10.3390/jcm11051152.
7. Epidemiology of Falling Fertility: The Contribution of Social, Environmental, and Genetic Forces. Aitken RJ, Norman RJ. Fertility and Sterility. 2025;:S0015-0282(25)00264-X. doi:10.1016/j.fertnstert.2025.04.048.
8. Population Decline: Where Demography, Social Science, and Biology Intersect. Aitken RJ. Reproduction (Cambridge, England). 2024;168(1):e240070. doi:10.1530/REP-24-0070.
9. Environmental Factors in Declining Human Fertility. Skakkebæk NE, Lindahl-Jacobsen R, Levine H, et al. Nature Reviews. Endocrinology. 2022;18(3):139-157. doi:10.1038/s41574-021-00598-8.
10. Fertility, Mortality, Migration, and Population Scenarios for 195 Countries and Territories From 2017 to 2100: A Forecasting Analysis for the Global Burden of Disease Study. Vollset SE, Goren E, Yuan CW, et al. Lancet (London, England). 2020;396(10258):1285-1306. doi:10.1016/S0140-6736(20)30677-2.
|
---
| tsitaat: |
**There is a statistical association between political preference on the left-right spectrum and number of children.** Conservative/right-leaning individuals have **higher fertility rates** than liberal/left-leaning individuals, with this gap **widening over time**. However, the available literature does not provide specific data on the association between political orientation and maternal age at first birth.
## Association Between Political Orientation and Number of Children
**Conservative/Republican individuals desire and have more children than liberal/Democratic individuals.** A nationally representative study of 67,557 American 12th graders from 1989-2019 found that Republicans consistently desired more children than Democrats, with this difference growing substantially over time—from 0.07 children in 1989-1993 to 0.29 children in 2014-2019.[1] In later periods, Republicans had higher probability of wanting four or more children and lower probability of eschewing parenthood entirely.[1]
**Actual completed fertility shows similar patterns.** Analysis of three large datasets (World Value Survey with 152,380 participants, Survey of Health, Ageing and Retirement in Europe with 65,912 participants, and General Social Survey of the United States with ~6,200 participants) demonstrated that right/conservative political attitudes are associated with higher average offspring numbers compared to intermediate attitudes.[2] In European and US surveys specifically, only the political right was associated with above-average number of children.[2]
**The pattern has evolved over time.** US data from 1972-2014 shows this association emerged during the 1990s. In the 1970s and 1980s, both political extremes (left and right) had reproductive advantages, but the fertility advantage for left-wing individuals vanished during the 1990s.[2]
**Differential fertility has measurable societal impacts.** Data from the General Social Survey indicate that higher-fertility individuals and their children are more conservative on "family values" issues. Over 2004-2018, opposition to same-sex marriage and abortion was 3-4 percentage points more prevalent than it would have been if traditional-family conservatism were independent of family size. As of 2018, differential fertility raised the number of US adults opposed to same-sex marriage by 17%, from 46.9 million to 54.8 million.[3]
## Mechanisms Underlying the Association
**Religiosity and gender attitudes explain much but not all of the gap.** Differences in religiosity and attitudes toward gender and childbearing explained Republican-Democrat fertility gaps before 2004. From 2004 onward, these factors attenuated but did not fully explain the partisan differences.[1]
**Parenthood itself may increase conservatism.** Cross-cultural evidence from 10 countries (n=2,610) and World Values Survey data (n=426,444) demonstrates that both parenthood and parental care motivation are associated with increased social conservatism globally. Most of the positive association between age and social conservatism is accounted for by parenthood status.[4]
**Family ideals directly map onto political attitudes.** Research supports Moral Politics Theory, which posits that individuals' ideals about parenting (strict-father versus nurturant-parent models) serve as conceptual templates for how society should function and predict whether one endorses conservative or progressive positions.[5][6]
## European Context
**Childless individuals vote differently in Europe.** Analysis of European Social Survey data from 20 countries (n=37,623) found that childless individuals voted for parties positioned at the Green-Alternative-Libertarian (GAL) pole rather than the Traditional-Authoritarian-Nationalist (TAN) pole of the ideological dimension.[7]
## Limitations Regarding Age at First Birth
The available literature does not provide specific statistical data on the relationship between political orientation and maternal age at first birth. While studies document that higher education is associated with later age at first birth, and that political orientation correlates with education levels, direct analysis of political preference and timing of first birth was not found in the searched literature.[8][9]
## References
1. Youth's Political Identity and Fertility Desires. Rackin HM, Gibson-Davis CM. Journal of Marriage and the Family. 2024;86(4):1132-1148. doi:10.1111/jomf.13000.
2. Political Attitude and Fertility: Is There a Selection for the Political Extreme?. Fieder M, Huber S. Frontiers in Psychology. 2018;9:2343. doi:10.3389/fpsyg.2018.02343.
3. Differential Fertility Makes Society More Conservative on Family Values. Vogl TS, Freese J. Proceedings of the National Academy of Sciences of the United States of America. 2020;117(14):7696-7701. doi:10.1073/pnas.1918006117.
4. Experimental and Cross-Cultural Evidence That Parenthood and Parental Care Motives Increase Social Conservatism. Kerry N, Al-Shawaf L, Barbato M, et al. Proceedings. Biological Sciences. 2022;289(1982):20220978. doi:10.1098/rspb.2022.0978.
5. A Moral House Divided: How Idealized Family Models Impact Political Cognition. Feinberg M, Wehling E. PloS One. 2018;13(4):e0193347. doi:10.1371/journal.pone.0193347.
6. Measuring Moral Politics: How Strict and Nurturant Family Values Explain Individual Differences in Conservatism, Liberalism, and the Political Middle. Feinberg M, Wehling E, Chung JM, Saslow LR, Melvær Paulin I. Journal of Personality and Social Psychology. 2020;118(4):777-804. doi:10.1037/pspp0000255.
7. Is There a "Childless Vote" in Europe?. Lönnqvist JE, Ilmarinen VJ. International Journal of Psychology : Journal International De Psychologie. 2023;58(6):512-517. doi:10.1002/ijop.12939.
8. Variations in Reproductive Events Across Life: A Pooled Analysis of Data From 505 147 Women Across 10 Countries. Human Reproduction (Oxford, England). 2019;34(5):881-893. doi:10.1093/humrep/dez015.
9. Increasingly Heterogeneous Ages at First Birth by Education in Southern European and Anglo-American Family-Policy Regimes: A Seven-Country Comparison by Birth Cohort. Rendall M, Aracil E, Bagavos C, et al. Population Studies. 2010;64(3):209-27. doi:10.1080/00324728.2010.512392.
|
---
| tsitaat: |
**There is a well-documented statistical association between household income and number of children, but the relationship is more complex than a simple threshold effect.** At the population level, **higher-income areas have lower birth rates**, and this negative gradient has **steepened dramatically since 2005** in the US. However, at the individual level, the direction of the association depends critically on **sex, the type of income measured, and whether confounders like opportunity cost are controlled**.
## The Population-Level Pattern: Higher Income, Fewer Births
A cross-sectional study of **86.7 million US births** (2000–2020) found that the association between county-level income and natality was essentially flat in 2000 (gradient: −0.061; 95% CI: −0.200 to 0.078) but became **strongly negative by 2020** (gradient: −0.572; 95% CI: −0.678 to −0.466).[1] The decline in natality was approximately **twice as large in the highest-income counties** compared with the lowest-income counties. Counterfactual modeling suggested that had natality inequality remained at its 2000 level, there would have been an additional **3.5 million births** (4.1% increase) over the study period.[1]
“The natality income gradient changed from −0.061 in 2000 to −0.572 in 2020, reflecting an increase in natality inequality. A negative gradient reflects that natality is lower in higher-income counties compared with lower-income counties.”
— Nick Turner, PhD1, et al.Federal Reserve Board of Governors, Washington, DC and other institutions
Importantly, this relationship appears **approximately linear across the income distribution** rather than showing a clear threshold. Birth rates decline progressively with each income ventile increase, without a sharp inflection point at a specific income level.[1]
## The Individual-Level Paradox: It Depends on Sex and What Is Measured
The relationship between income and fertility differs substantially by sex and by the type of income measured, based on US Census Survey of Income and Program Participation data (2014):[2]
- **Men's personal income** is **positively** associated with fertility — higher-earning men have more children
- **Women's personal income** is **negatively** associated with fertility — higher-earning women have fewer children
- **Family income (net of personal income)** is **positively** associated with fertility for women — women with higher-earning partners have more children
- **Family net worth** is **negatively** associated with fertility for both sexes
This paradox is explained by the **opportunity cost of childbearing**, which falls disproportionately on women. When the "net price of a child" (including opportunity cost of the mother's time) is statistically controlled, the pure income effect on fertility becomes **positive and significant**. Without this control, the income effect appears negative.[3]
## Swedish Longitudinal Evidence: The Gradient Is Shifting
A Swedish register-based study of cohorts born 1940–1970 using lifetime accumulated income found a **strong positive gradient** between income and fertility for men across all cohorts, and a **gradual transformation from negative to positive** for women in more recent cohorts.[4] For men, fertility increased **monotonically** with income. For women, the positive gradient was primarily driven by very low fertility among women with the lowest accumulated incomes. Individuals with 2–4 children had the highest accumulated incomes, while **childless men and women had substantially lower lifetime incomes**.[4]
## Fecundability: A Graded Relationship Without a Sharp Threshold
Studies examining biological fecundability (per-cycle probability of conception) show a **graded, dose-response relationship** with household income rather than a discrete threshold:
- In a Dutch cohort, household income **[5]
- In a Danish cohort of 10,475 women, compared to household income >65,000 DKK/month (~€8,700), fecundability was progressively lower at [6]
- In a North American cohort of 8,654 women, household income [7]
The following figure illustrates the graded association between poverty, education, and household income with fecundability:
Figure 1
Associations of Poverty, Educational Level of Women and Men, and Household Income With Fecundability
undefined
## Summary
Rather than a single income threshold, the evidence points to a **continuous, approximately linear negative gradient** between area-level income and birth rates that has steepened over time.[1] At the individual level, the relationship is **sex-dependent**: positive for men's income, negative for women's personal income, but positive for partner/family income — reflecting the **opportunity cost trade-off** women face between career advancement and childbearing.[2][3] The literature from multiple countries consistently shows that the relationship is graded rather than threshold-based, with economic insecurity at lower income levels and opportunity costs at higher income levels both contributing to reduced fertility through different mechanisms.[8]
## References
1. Association Between County-Level Natality and Income in the US, 2000-2020. Turner N, Robbins K. JAMA Pediatrics. 2023;177(2):198-202. doi:10.1001/jamapediatrics.2022.4814.
2. Sex Differences in the Association of Family and Personal Income and Wealth With Fertility in the United States. Hopcroft RL. Human Nature (Hawthorne, N.Y.). 2019;30(4):477-495. doi:10.1007/s12110-019-09354-4.
3. The Income--Fertility Relationship: Effect of the Net Price of a Child . Borg MO. Demography. 1989;26(2):301-10.
4. The Relationship Between Life-Course Accumulated Income and Childbearing of Swedish Men and Women Born 1940-70. Kolk M. Population Studies. 2023;77(2):197-215. doi:10.1080/00324728.2022.2134578.
5. Poverty and Social Disadvantage in Women and Men and Fertility Outcomes. Boxem AJ, Mulders AGMGJ, van Rossum I, et al. JAMA Network Open. 2025;8(9):e2532741. doi:10.1001/jamanetworkopen.2025.32741.
6. Socioeconomic Status and Fecundability in a Danish Preconception Cohort. Jørgensen MD, Mikkelsen EM, Hatch EE, et al. Human Reproduction (Oxford, England). 2023;38(6):1183-1193. doi:10.1093/humrep/dead077.
7. Association of Income and Education With Fecundability in a North American Preconception Cohort. Schrager NL, Wesselink AK, Wang TR, et al. Annals of Epidemiology. 2020;50:41-47.e1. doi:10.1016/j.annepidem.2020.07.004.
8. Wealth, Fertility and Adaptive Behaviour in Industrial Populations. Stulp G, Barrett L. Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 2016;371(1692):20150153. doi:10.1098/rstb.2015.0153.
|
---
| tsitaat: |
**There is a strong and well-documented statistical association between economic crises and fertility decline.** Fertility is **pro-cyclical** in modern economies — it rises during economic expansions and falls during downturns.[1][2] Crises also **postpone first births**, particularly among young adults under 30, and in some cases this postponement becomes **permanent childlessness**.[3][4]
## Economic Recessions and Birth Rates
**The relationship between economic conditions and fertility has fundamentally changed over time.** Before 1970, fertility was actually counter-cyclical (good economic times were associated with lower fertility), but since then it has become **pro-cyclical**, with good economic times associated with higher fertility.[2] This shift means that modern recessions consistently depress birth rates.
The effects operate through several mechanisms: **economic uncertainty, falling income, housing market declines, rising enrollment in higher education, and declining marriage rates**.[1] Unemployment is the single most important economic indicator — a multinational analysis of 30 OECD countries (1976–2014) found that increases in unemployment significantly reduced fertility rates in both Western European (−0.00256; p [5]
However, the aggregate effects are typically **relatively small (a few percentage points) and of short duration**, primarily influencing the timing rather than the quantum of childbearing. Major long-term fertility shifts often continue seemingly uninterrupted during recessions — including during the Great Depression of the 1930s and the oil shock crises of the 1970s.[1]
## Impact on Age at First Birth and Postponement
**Economic crises disproportionately delay first births among young adults.** A study of 14 European countries (1970–2005) found that adverse economic conditions and high unemployment **significantly reduce first birth hazards among men and women below age 30**, particularly among the higher educated. After age 30, economic context continued to affect men's first birth hazards but **not women's**, suggesting that women over 30 are less willing to further delay childbearing regardless of economic conditions.[4]
**Critically, postponement during recessions can become permanent.** Using over 140 million US birth records (1975–2010), Currie and Schwandt found that women in their **early 20s** are most affected. A one percentage point increase in the average unemployment rate experienced between ages 20–24 reduced short-run fertility by **6 conceptions per 1,000 women**, but when these women were followed to age 40, the total loss grew to **14.2 conceptions per 1,000 women**. This long-run effect was driven largely by women who **remained permanently childless** — they did not have first births or any higher-order births.[3]
## The 2008 Great Recession
The Great Recession brought a **sharp halt to the previous decade of rising fertility rates** in most developed countries.[1] In the United States, the total fertility rate declined steadily from 2007, reaching **1.73 children in 2018** — the lowest level since the 1970s.[6] Total intended parity also declined (from 2.26 in 2006–2010 to 2.16 in 2013–2017), and the proportion intending to remain childless increased, indicating that the decline was not purely a timing effect.[6] The mean age at first birth in the US rose from approximately 25 in 2007 to **27.3 in 2021**.[7]
## The COVID-19 Pandemic
The COVID-19 pandemic produced a **sharp but heterogeneous fertility decline**. Across 24 European countries, a **−14.1% decline in live births** was observed in January 2021 (9–10 months after the first wave peaks and lockdowns), with the duration of lockdowns being the strongest predictor of this decline.[8] Southern European countries were particularly affected: Italy (−9.1%), Spain (−8.4%), and Portugal (−6.6%).[9]
In the US, the initial response differed by nativity: **60% of the 2020 fertility decline was driven by reductions in births to foreign-born mothers** (who comprised only 22% of births). Among US-born mothers, a surprising **"baby bump"** occurred — births fell by 31,000 in 2020 but increased by 71,000 in 2021, marking the first reversal in declining fertility since the Great Recession. This bump was most pronounced for **first births and women under 25**, suggesting some women started families earlier during the pandemic.[10]
In Italy, the pandemic's economic consequences directly affected fertility plans: individuals who suffered negative income shocks or had negative expectations about future income and occupation were **more likely to abandon their pre-pandemic fertility plans**, and this effect persisted across both early and later phases of the pandemic.[11]
## Wars and Geopolitical Crises
**Armed conflicts generally reduce fertility during the active phase**, followed by a post-conflict rebound.[12] Mechanisms include spousal separation, reduced marriage rates, lower fecundity, and increased spontaneous abortion (especially when famine coexists).[12] In Cambodia, fertility decreased by approximately **one-third** from pre-civil war levels during 1975–79.[12]
A recent study on Ukraine found that **geopolitical uncertainty following the Crimean crisis (2014) significantly reduced fertility rates**, with households exhibiting precautionary behavior in their fertility decisions. In a low-fertility regime, geopolitical uncertainty proved to be a crucial predictor of fertility behavior.[13]
The Rwandan genocide (1994) demonstrated heterogeneous effects: women who lost a child during the genocide showed a strong **child replacement effect** (increased subsequent fertility), while those who experienced sibling death had **lower post-genocide fertility** in both the short and long run.[14]
## A Meta-Analytic Perspective on Employment Instability
A European meta-analysis synthesizing research findings on employment instability and fertility confirmed a **nonnegligible negative effect** overall, with important nuances:[15]
- **Men's unemployment** is more detrimental to fertility than men's time-limited employment
- **Women's fixed-term contracts** are the most detrimental form of employment instability for fertility
- The negative effect has become **stronger over time** and is **more severe in Southern European countries**, where social protection for families and the unemployed is least generous
- Failing to account for income and partner characteristics leads to an **overestimation** of the negative effect
## Summary
A systematic review of 50 studies on fertility after disasters found an **overall negative impact** on fertility across disaster types, though weather-related physical disasters occasionally produced small increases.[16] The evidence consistently shows that crises reduce fertility primarily through postponement of first births among young adults, with the degree of impact modulated by the strength of social safety nets and family policies. The most concerning finding is that recession-induced postponement among women in their early 20s often does not fully recover, contributing to **permanently lower completed fertility**.[3]
## References
1. Economic Recession and Fertility in the Developed World. Sobotka T, Skirbekk V, Philipov D. Population and Development Review. 2011;37(2):267-306. doi:10.1111/j.1728-4457.2011.00411.x.
2. The Changing Relationship Between Unemployment and Total Fertility. Karaman Örsal DD, Goldstein JR. Population Studies. 2018;72(1):109-121. doi:10.1080/00324728.2017.1404624.
3. Short- And Long-Term Effects of Unemployment on Fertility. Currie J, Schwandt H. Proceedings of the National Academy of Sciences of the United States of America. 2014;111(41):14734-9. doi:10.1073/pnas.1408975111.
4. Economic Recession and First Births in Europe: Recession-Induced Postponement and Recuperation of Fertility in 14 European Countries Between 1970 and 2005. Neels K, Theunynck Z, Wood J. International Journal of Public Health. 2013;58(1):43-55. doi:10.1007/s00038-012-0390-9.
5. Influence of Obesity and Unemployment on Fertility Rates: A Multinational Analysis of 30 Countries From 1976 to 2014. König-Castillo DM, Ott J, König D, et al. Journal of Clinical Medicine. 2022;11(5):1152. doi:10.3390/jcm11051152.
6. Recent Trends in U.S. Childbearing Intentions. Hartnett CS, Gemmill A. Demography. 2020;57(6):2035-2045. doi:10.1007/s13524-020-00929-w.
7. Management of Pregnancy (2023). Colleen C. Blosser MSN RN, Michael Bybel DO FAAFP, Alicia Christy MD MHSCR, et al. Department of Veterans Affairs.
8. Impact of the First Wave of the COVID-19 Pandemic on Birth Rates in Europe: A Time Series Analysis in 24 Countries. Pomar L, Favre G, de Labrusse C, et al. Human Reproduction (Oxford, England). 2022;37(12):2921-2931. doi:10.1093/humrep/deac215.
9. Early Assessment of the Relationship Between the COVID-19 Pandemic and Births in High-Income Countries. Aassve A, Cavalli N, Mencarini L, Plach S, Sanders S. Proceedings of the National Academy of Sciences of the United States of America. 2021;118(36):e2105709118. doi:10.1073/pnas.2105709118.
10. The COVID-19 Baby Bump in the United States. Bailey MJ, Currie J, Schwandt H. Proceedings of the National Academy of Sciences of the United States of America. 2023;120(34):e2222075120. doi:10.1073/pnas.2222075120.
11. Fertility Plans in the Early Times of the COVID-19 Pandemic: The Role of Occupational and Financial Uncertainty in Italy. Luppi F, Arpino B, Rosina A. PloS One. 2022;17(12):e0271384. doi:10.1371/journal.pone.0271384.
12. The Effects of Armed Conflict on the Health of Women and Children. Bendavid E, Boerma T, Akseer N, et al. Lancet (London, England). 2021;397(10273):522-532. doi:10.1016/S0140-6736(21)00131-8.
13. Fertility Behaviour Under Geopolitical Uncertainty: Evidence From Ukraine. Saha J. Economics and Human Biology. 2026;61:101594. doi:10.1016/j.ehb.2026.101594.
14. The Effects of Conflict on Fertility: Evidence From the Genocide in Rwanda. Kraehnert K, Brück T, Di Maio M, Nisticò R. Demography. 2019;56(3):935-968. doi:10.1007/s13524-019-00780-8.
15. Employment Instability and Fertility in Europe: A Meta-Analysis. Alderotti G, Vignoli D, Baccini M, Matysiak A. Demography. 2021;58(3):871-900. doi:10.1215/00703370-9164737.
16. Human Fertility After a Disaster: A Systematic Literature Review. Lee DS, Batyra E, Castro A, Wilde J. Proceedings. Biological Sciences. 2023;290(1998):20230211. doi:10.1098/rspb.2023.0211.
|
---
| tsitaat: |
Among the material and economic factors influencing first births, **housing costs and housing market conditions** are the single most impactful material asset-related factor, with expensive housing markets delaying first births by **3–4 years** even after controlling for education, ethnicity, and labor force participation.[1] However, **education and women's labor force participation** remain the strongest overall predictors of reproductive timing, with housing operating as an important but secondary factor within a complex decision-making structure.[2]
## Hierarchy of Factors Affecting First Birth Timing
A systematic review following PRISMA methodology identified the central reasons for postponement of first births in Western societies, ranked by strength of evidence:[2]
1. **Women's education and labor force participation** — the strongest and most consistently documented factor. Women with low education had **7-fold higher odds** of first birth before age 24 compared to highly educated women (OR 7.0; 95% CI: 5.3–9.3). The "parenthood wage penalty" — predicted income loss from early childbearing — is a powerful driver of delayed fertility, particularly among high-SES individuals.[3][4]
2. **Housing conditions and costs** — the most important material asset factor (discussed in detail below).
3. **Economic uncertainty and employment security** — the husband's employment security and stable housing arrangements appear to be the **most important factors** for a married couple's fertility decisions in low-fertility settings like South Korea.[5]
4. **Partnership formation and stability** — partnership changes and delayed marriage directly delay first births.[2]
5. **Contraceptive access and value changes** — enabling factors that interact with all of the above.[2]
## Housing: The Dominant Material Factor
**Housing costs and mortgage burden**
Living in an expensive housing market delays first births by **3–4 years** after controlling for education, ethnicity, and labor market participation, based on analysis of 25 US metropolitan areas using American Community Survey data (2006–2008).[1] However, the relatively modest fit of individual-level models suggests that housing is one component within a complex decision-making structure involving fertility, labor force participation, and housing market entry simultaneously.[1]
**Mortgage debt specifically reduces fertility intentions.** A Chinese study of 7,512 adults found that housing mortgage burden was **negatively associated** with fertility intention, and this was one of the primary mechanisms through which housing status affected childbearing decisions.[6] In Europe, the economic consequences of housing costs operate through similar channels — individuals who suffered negative income shocks (often housing-related) were more likely to **abandon pre-existing fertility plans**.[7]
**Homeownership and the transition to parenthood**
Traditionally, homeownership was positively linked to the transition to parenthood — couples preferred to become homeowners before having their first child. However, British longitudinal data (1991–2016) shows this relationship has **fundamentally changed**: the likelihood of becoming a parent has declined among homeowners while remaining stable among private renters, making the two groups increasingly similar in their likelihood of entering parenthood. This reflects the reality of "Generation Rent," where rising housing unaffordability has undermined the traditional sequencing of homeownership before parenthood.[8]
**Housing size and dwelling type**
Longitudinal US data supports the prediction that **higher fertility is associated with larger dwellings**.[9] In tight housing markets, apartment dwellers reduced their fertility while house dwellers did not, consistent with the utility-cost theory of fertility — the marginal cost of an additional child is higher in constrained living spaces.[9] Increasing population density at the macro level is also robustly associated with declining fertility rates across 174 countries over 69 years (1950–2019), even after controlling for socioeconomic variables.[10]
## Financial Hardship Across the Life Course
A North American preconception cohort (PRESTO, n=6,377) found that **adult financial hardship** was the most sensitive period for fertility effects, reducing fecundability by 17% (FR: 0.83; 95% CI: 0.77–0.90). Critically, the effect was **cumulative**: individuals who experienced financial hardship in both childhood and adulthood had even lower fecundability (FR: 0.77; 95% CI: 0.64–0.93) than those experiencing adult hardship alone.[13]
## Summary Table
| Factor | Effect on First Birth Timing | Effect on Number of Children | Strength of Evidence | References |
|---|---|---|---|---|
| Women's education | Strongest predictor; delays first birth by 5–10+ years between lowest and highest groups | Higher education → fewer children | Very strong (multiple large cohorts) | [1-2] |
| Housing costs/mortgage | Delays first birth by 3–4 years in expensive markets | Mortgage burden reduces fertility intentions | Strong (multiple countries) | [3-4] |
| Housing size/type | Apartment living constrains fertility in tight markets | Larger dwellings associated with higher fertility | Moderate (older studies) | [5] |
| Employment security (husband's) | Delays first birth when insecure | Among the most important factors for couple fertility | Strong (European/Asian data) | [6-7] |
| Financial opportunity cost (women's income) | Higher potential income → later first birth | Higher personal income → fewer children for women | Strong (Finnish register data, n=47,678) | [8-9] |
| Homeownership | Traditionally positive; now weakening | Declining association in "Generation Rent" | Moderate-strong (UK longitudinal) | [10] |
| Cumulative financial hardship | Not directly studied for timing | Reduces fecundability by 17–23% | Moderate (preconception cohort) | [11] |
The key insight from the literature is that these factors do not operate independently — they form an interconnected decision-making structure where **education drives labor force participation, which drives income, which determines housing affordability, which influences fertility timing**.[2][4] Housing is the most important single material asset factor, but it is embedded within this broader socioeconomic cascade.
## References
1. Do Women Delay Family Formation in Expensive Housing Markets?. Clark WA. Demographic Research. 2012;27(1):1-24. doi:10.4054/DemRes.2012.27.1.
2. Why Do People Postpone Parenthood? Reasons and Social Policy Incentives. Mills M, Rindfuss RR, McDonald P, te Velde E. Human Reproduction Update. 2011 Nov-Dec;17(6):848-60. doi:10.1093/humupd/dmr026.
3. Socioeconomic Position and Reproduction: Findings From the Australian Longitudinal Study on Women's Health. Holowko N, Jones M, Tooth L, Koupil I, Mishra GD. Maternal and Child Health Journal. 2018;22(12):1713-1724. doi:10.1007/s10995-018-2567-1.
4. Financial Opportunity Costs and Deaths Among Close Kin Are Independently Associated With Reproductive Timing in a Contemporary High-Income Society. Berg V, Lawson DW, Rotkirch A. Proceedings. Biological Sciences. 2020;287(1919):20192478. doi:10.1098/rspb.2019.2478.
5. Socioeconomic Differentials in Fertility in South Korea. Lim S. Demographic Research. 2021 Jan-Jun;44:941-978. doi:10.4054/demres.2021.44.39.
6. Does Inhabitant's Fertility Intention Respond to Housing Status in the Urban Built Environment: Evidence From China. Zhuang X, Li Q, Su T, et al. Frontiers in Public Health. 2025;13:1328329. doi:10.3389/fpubh.2025.1328329.
7. Fertility Plans in the Early Times of the COVID-19 Pandemic: The Role of Occupational and Financial Uncertainty in Italy. Luppi F, Arpino B, Rosina A. PloS One. 2022;17(12):e0271384. doi:10.1371/journal.pone.0271384.
8. The Changing Association Between Homeownership and the Transition to Parenthood. Tocchioni V, Berrington A, Vignoli D, Vitali A. Demography. 2021;58(5):1843-1865. doi:10.1215/00703370-9420322.
9. The Relationship Between Apartment Living and Fertility for Blacks, Mexican-Americans, and Other Americans in Racine, Wisconsin. Curry JP, Scriven GD. Demography. 1978;15(4):477-85.
10. Increasing Population Densities Predict Decreasing Fertility Rates Over Time: A 174-Nation Investigation. Rotella A, Varnum MEW, Sng O, Grossmann I. The American Psychologist. 2021;76(6):933-946. doi:10.1037/amp0000862.
11. Sex Differences in the Association of Family and Personal Income and Wealth With Fertility in the United States. Hopcroft RL. Human Nature (Hawthorne, N.Y.). 2019;30(4):477-495. doi:10.1007/s12110-019-09354-4.
12. The Reproductive Ecology of Industrial Societies, Part II : The Association Between Wealth and Fertility. Stulp G, Sear R, Schaffnit SB, Mills MC, Barrett L. Human Nature (Hawthorne, N.Y.). 2016;27(4):445-470. doi:10.1007/s12110-016-9272-9.
13. Life Course Financial Hardship and Fecundability in a North American Preconception Cohort Study. Hoffman MN, Ncube CN, Murray EJ, et al. Epidemiology (Cambridge, Mass.). 2025;:00001648-990000000-00397. doi:10.1097/EDE.0000000000001900.
14. Variations in Reproductive Events Across Life: A Pooled Analysis of Data From 505 147 Women Across 10 Countries. Human Reproduction (Oxford, England). 2019;34(5):881-893. doi:10.1093/humrep/dez015.
|
---
| tsitaat: |
**Substance use has well-documented statistical associations with fertility outcomes, though the effects vary by substance type and sex.** **Tobacco smoking** has the strongest and most consistent negative effect, increasing infertility risk by **60% (OR 1.60)** and causing conception delays of **54% longer** in smokers versus non-smokers.[1][2] **Alcohol** shows a dose-dependent negative association with female fecundability, with heavy drinking (>6 drinks/week) reducing conception odds by **40–50%**.[3][4] **Cannabis** effects are more mixed, with some studies showing reduced fecundability while others show no association.[5][6]
## Tobacco Smoking
**Effect on fertility and fecundability**
Tobacco smoking has the most robust evidence for negative reproductive effects. According to the American Society for Reproductive Medicine (ASRM), a meta-analysis of 12 studies (10,928 exposed vs. 19,179 unexposed women) found:[1][2]
- Overall infertility risk: **OR 1.60 (95% CI: 1.34–1.91)**
- Conception delay >1 year: **OR 1.42 (95% CI: 1.27–1.58)** in cohort studies
- Infertility in case-control studies: **OR 2.27 (95% CI: 1.28–4.02)**
- Conception delay >12 months was **54% higher** for smokers than non-smokers
- **Dose-dependent effect**: increasing delay correlates with increasing daily cigarette consumption
**Effect on number of children and age at first birth**
A Swiss population-based study (n=6,711) found paradoxical associations:[7]
- **Fewer children**: Current female smokers had 1.38 children vs. 1.58 for never-smokers (p[1] Anti-Müllerian hormone (AMH) levels are **44% lower** in current smokers compared to never-smokers, and AMH declines **21% faster per year** in smokers.[1] In men, smoking affects spermatogenesis through oxidative stress and apoptosis in testicular tissue.[8]
## Alcohol
**Effect on female fecundability**
A systematic review and dose-response meta-analysis of 19 studies (98,657 women) found:[4]
- Overall fecundability reduction: **RR 0.87 (95% CI: 0.78–0.95)** for drinkers vs. non-drinkers
- Light drinkers (≤12.5 g/day): **RR 0.89 (95% CI: 0.82–0.97)**
- Moderate-heavy drinkers (>12.5 g/day): **RR 0.77 (95% CI: 0.61–0.94)**
- **Linear dose-response**: Each 12.5 g/day increase associated with RR 0.98 (95% CI: 0.97–0.99)
The timing of alcohol consumption within the menstrual cycle matters significantly. Heavy drinking (>6 drinks/week) during the **luteal phase** reduced fecundability by **49% (FOR 0.51; 95% CI: 0.29–0.89)**, and during the **ovulatory window** by **61% (FOR 0.39; 95% CI: 0.19–0.72)**.[3]
**Effect on male fertility**
In contrast to women, pooled data from Danish and North American preconception cohorts (2,679 couples) found **little evidence** of an association between male alcohol consumption and reduced fecundability.[9] However, chronic alcohol dependence in males is associated with lower sperm counts, motility, morphology, seminal fluid volume, and testosterone levels.[5]
**Effect on number of children**
A 33-year Finnish twin follow-up study (>3,500 twin pairs) found a **U-shaped relationship**:[10]
- Both **abstinence** and **heavier drinking** at ages 18–25 predicted lifetime childlessness
- Among those who had children, heavier drinking predicted **smaller family size**
- These associations persisted in within-pair analyses of monozygotic twins, ruling out familial confounds
**Effect on reproductive timing**
Alcohol use disorder (AUD) is associated with **delayed reproduction** or no reproduction, while parental AUD is associated with **early reproduction**.[11] This suggests that AUD may delay reproductive onset through biological impairment or psychosocial mediators such as delays in role transitions.
## Cannabis (Marijuana)
**Effect on fertility**
The evidence on cannabis is more mixed than for tobacco or alcohol:[5][12]
- One study found infertility prevalence increased in ovulatory cannabis users: **RR 1.7 (95% CI: 1.0–3.0)**
- Men who smoke cannabis have **29% lower sperm counts** with a dose-dependent effect
- However, data from the National Survey of Family Growth and PRESTO cohort showed **no association** between male or female cannabis use and time to pregnancy
A prospective cohort study of 1,228 women with a history of pregnancy loss found preconception cannabis use was associated with **reduced fecundability (FOR 0.59; 95% CI: 0.38–0.92)**, despite increased intercourse frequency.[6]
**Biological mechanisms**
Cannabis affects the endocannabinoid system, which plays a role in regulating reproduction. Effects include:[12][13]
- Altered reproductive hormones and menstrual cyclicity
- Disturbed folliculogenesis and ovulation
- In males: erectile dysfunction, abnormal spermatogenesis, testicular atrophy
- In females: abnormal embryo implantation and development
The ASRM and ACOG recommend that women who are pregnant or may become pregnant should **discontinue cannabis use** due to adverse effects on fetal neurodevelopment.[5]
## Other Recreational Drugs
**Opioids, amphetamines, and cocaine**
Substance abuse is a recognized cause of male hypogonadism:[8]
- **Opioids** reduce testosterone production by interfering with hypothalamic-pituitary function
- **Anabolic-androgenic steroids** suppress gonadotropin secretion, causing hypogonadism
- **Amphetamines** alter spermatogenesis through oxidative stress
One study found that women who had used **marijuana regularly** or **cocaine** actually had **shorter time to conception** than non-users — a counterintuitive finding that may reflect confounding by sexual behavior patterns rather than a biological effect.[14]
The use of non-prescription and recreational drugs before conception is associated with reduced fertility in both men and women, and during pregnancy is associated with increased risk of fetal death, low birth weight, and preterm birth.[15]
## Summary Table
| Substance | Effect on Female Fertility | Effect on Male Fertility | Effect on Number of Children | Effect on Age at First Birth | References |
|---|---|---|---|---|---|
| **Tobacco** | OR 1.60 for infertility; 54% longer time to conception | Reduced sperm parameters; oxidative damage | Fewer children (1.38 vs. 1.58) | Earlier first birth (26.7 vs. 26.9 years) |[1-3] |
| **Alcohol (heavy)** | RR 0.77 for fecundability; 40–50% reduction in luteal/ovulatory phases | Chronic use: lower sperm count, motility, testosterone | U-shaped: abstinence and heavy use both predict fewer children | AUD predicts delayed reproduction | [4-6] |
| **Cannabis** | Mixed: RR 1.7 for infertility in some studies; no effect in others | 29% lower sperm counts (dose-dependent) | Limited data | Limited data | [7-8] |
| **Opioids** | Limited data | Hypogonadism; reduced testosterone | Limited data | Limited data | [9] |
| **Cocaine** | Paradoxically shorter time to conception (likely confounded) | Limited data | Limited data | Limited data | [10] |
[5][3][4][9][7][6][8][10][14][11]
## Key Clinical Implications
The ASRM recommends that couples attempting pregnancy should be counseled to:[5][1][15]
- **Avoid tobacco smoking** — the most consistently harmful substance for fertility
- **Limit alcohol** to moderate levels (<2 drinks/day); higher consumption should be avoided
- **Discontinue cannabis** — particularly for women who are pregnant or may become pregnant
- **Stop all recreational drug use** before conception
Importantly, substance use effects on fertility are often reversible with cessation, making preconception counseling a critical intervention point. [8][18]
## References
1. Tobacco or Marijuana Use and Infertility: A Committee Opinion. Fertility and Sterility. 2024;121(4):589-603. doi:10.1016/j.fertnstert.2023.12.029.
2. Smoking and Infertility. Fertility and Sterility. 2006;86(5 Suppl 1):S172-7. doi:10.1016/j.fertnstert.2006.08.018.
3. The Association Between Alcohol Intake and Fecundability During Menstrual Cycle Phases. Anwar MY, Marcus M, Taylor KC. Human Reproduction (Oxford, England). 2021;36(9):2538-2548. doi:10.1093/humrep/deab121.
4. Female Alcohol Consumption and Fecundability: A Systematic Review and Dose-Response Meta-Analysis. Fan D, Liu L, Xia Q, et al. Scientific Reports. 2017;7(1):13815. doi:10.1038/s41598-017-14261-8.
5. Optimizing Natural Fertility: A Committee Opinion. Penzias A, Azziz R, Bendikson K, et al. Fertility and Sterility. 2022;117(1):53-63. doi:10.1016/j.fertnstert.2021.10.007.
6. Cannabis Use While Trying to Conceive: A Prospective Cohort Study Evaluating Associations With Fecundability, Live Birth and Pregnancy Loss. Mumford SL, Flannagan KS, Radoc JG, et al. Human Reproduction (Oxford, England). 2021;36(5):1405-1415. doi:10.1093/humrep/deaa355.
7. Impact of Smoking on Fertility and Age of Menopause: A Population-Based Assessment. Oboni JB, Marques-Vidal P, Bastardot F, Vollenweider P, Waeber G. BMJ Open. 2016;6(11):e012015. doi:10.1136/bmjopen-2016-012015.
8. Substance Abuse and Male Hypogonadism. Duca Y, Aversa A, Condorelli RA, Calogero AE, La Vignera S. Journal of Clinical Medicine. 2019;8(5):E732. doi:10.3390/jcm8050732.
9. Male Alcohol Consumption and Fecundability. Høyer S, Riis AH, Toft G, et al. Human Reproduction (Oxford, England). 2020;35(4):816-825. doi:10.1093/humrep/dez294.
10. Alcohol Consumption at Age 18-25 and Number of Children at a 33-Year Follow-Up: Individual and Within-Pair Analyses of Finnish Twins. Rose RJ, Latvala A, Silventoinen K, Kaprio J. Alcoholism, Clinical and Experimental Research. 2022;46(8):1552-1564. doi:10.1111/acer.14886.
11. Alcohol Use Disorder and Parental Alcohol Use Disorder as Predictors of Reproductive Timing. Blake A, Smyth H, Sternberg A, Waddell J, Chassin L. Journal of Studies on Alcohol and Drugs. 2020;81(5):575-583.
12. Impact of Cannabinoids on Pregnancy, Reproductive Health, and Offspring Outcomes. Lo JO, Hedges JC, Girardi G. American Journal of Obstetrics and Gynecology. 2022;227(4):571-581. doi:10.1016/j.ajog.2022.05.056.
13. Cannabis and Cannabinoids in Reproduction and Fertility: Where We Stand. Fonseca BM, Rebelo I. Reproductive Sciences (Thousand Oaks, Calif.). 2022;29(9):2429-2439. doi:10.1007/s43032-021-00588-1.
14. Fertility and Use of Cigarettes, Alcohol, Marijuana, and Cocaine. Joesoef MR, Beral V, Aral SO, Rolfs RT, Cramer DW. Annals of Epidemiology. 1993;3(6):592-4. doi:10.1016/1047-2797(93)90080-n.
15. Preconception Lifestyle Advice for People With Infertility. Boedt T, Vanhove AC, Vercoe MA, et al. The Cochrane Database of Systematic Reviews. 2021;4:CD008189. doi:10.1002/14651858.CD008189.pub3.
16. Does Moderate Alcohol Consumption Affect Fertility? Follow Up Study Among Couples Planning First Pregnancy. Jensen TK, Hjollund NH, Henriksen TB, et al. BMJ (Clinical Research Ed.). 1998;317(7157):505-10. doi:10.1136/bmj.317.7157.505.
17. Adult and Prenatal Exposures to Tobacco Smoke as Risk Indicators of Fertility Among 430 Danish Couples. Jensen TK, Henriksen TB, Hjollund NH, et al. American Journal of Epidemiology. 1998;148(10):992-7. doi:10.1093/oxfordjournals.aje.a009576.
18. Smoke, Alcohol and Drug Addiction and Male Fertility. Sansone A, Di Dato C, de Angelis C, et al. Reproductive Biology and Endocrinology : RB&E. 2018;16(1):3. doi:10.1186/s12958-018-0320-7.
|
_________________
All it took was for a lot of seemingly decent people to put the wrong person in power, and then pay for their innocent choice. |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
RedFusion
HV kasutaja

liitunud: 14.12.2009
|
|
| Kommentaarid: 8 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
7 |
|
| tagasi üles |
|
|
Betamax
HV Guru

liitunud: 29.05.2003
|
|
| Kommentaarid: 754 loe/lisa |
Kasutajad arvavad: |
|
:: |
1 :: |
1 :: |
566 |
|
| tagasi üles |
|
|
mikk36
HV Guru

liitunud: 21.02.2004
|
|
15.05.2026 11:35:16
Re: Iibe ja demograafia teema (lisatud küsitlus) |
|
|
|
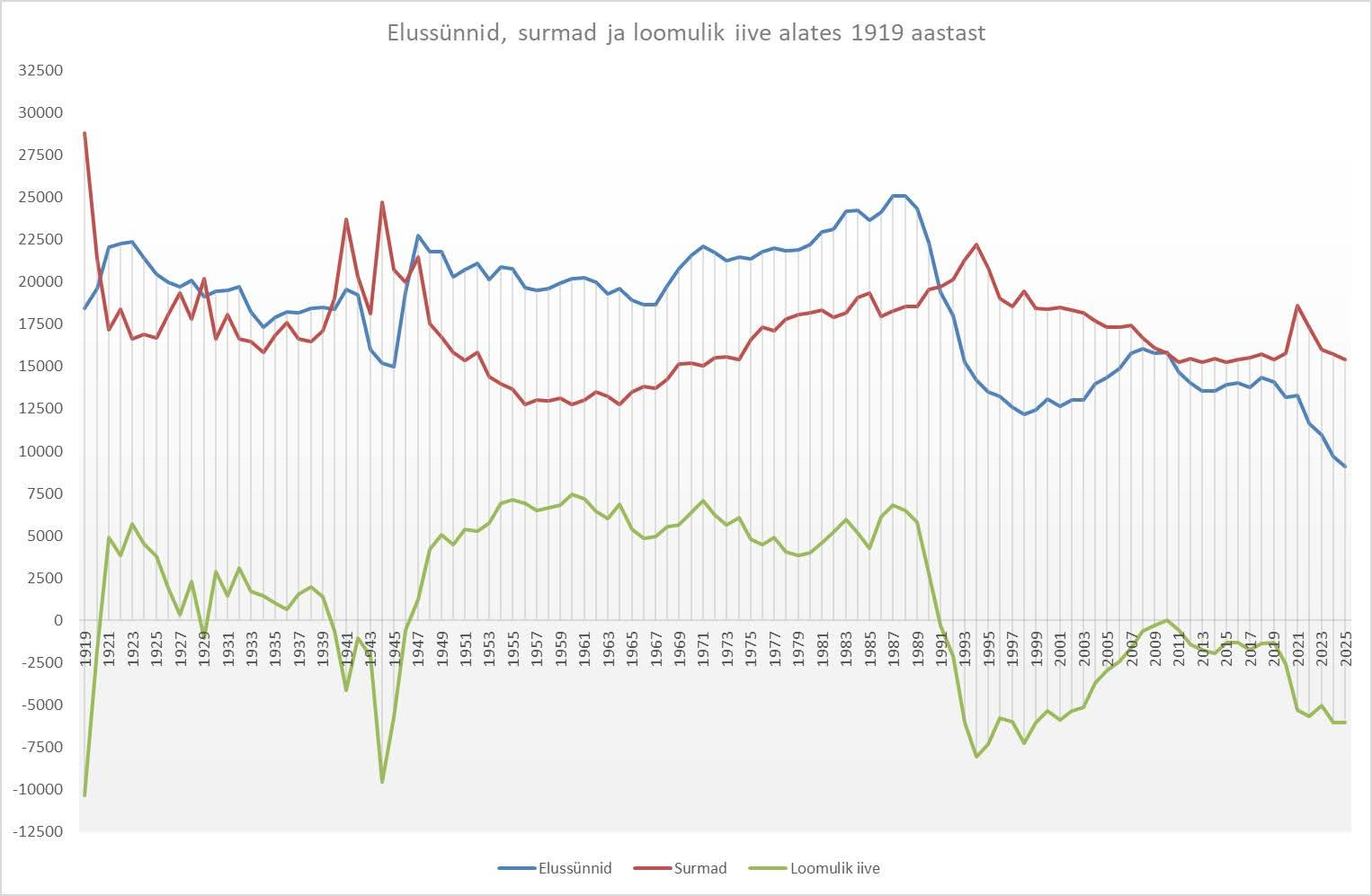
Miks on iive positiivne just nõukogude võimu all olemise ajal?
|
|
| Kommentaarid: 85 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
2 :: |
78 |
|
| tagasi üles |
|
|
Tbit
HV Guru
liitunud: 27.04.2004
|
|
15.05.2026 12:25:30
Re: Iibe ja demograafia teema (lisatud küsitlus) |
|
|
| mikk36 kirjutas: |
|
Miks on iive positiivne just nõukogude võimu all olemise ajal? |
"Vene aeg oli hea/parem . . ."
Statistilises vaates teevad inimesed lapsi ikkagi siis kui selleks on stabiilne väljavaade.
_________________
DVD is da 4483MB :-/)
|OSTAN|-> T43 pikk jahutus |
|
| Kommentaarid: 265 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
3 :: |
230 |
|
| tagasi üles |
|
|
netcat
Kreisi kasutaja

liitunud: 13.01.2010
|
|
15.05.2026 12:39:55
|
|
|
| Kui sa tead, et traktor tõmbab alati teki peale ja kedagi tööta ei jäeta... kapitalismis on lapsed töövõtjale puue. Sotsialismuses on need argument, millega võita eelisõigusi. Sa võtsid need käekõrvale ja läksid, "kuhu vaja", jalgu trampima, et sulle kui "kangelasemale" "eraldataks" mida vaja... Ja vahel antigi, vastavalt ajastule siis mida, lisatoidunorm, elamispind, puhkusetuusik vms
|
|
| Kommentaarid: 7 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
7 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
napoleon
Unknown virus

liitunud: 08.12.2008
|
|
15.05.2026 13:33:47
|
|
|
| Tanel kirjutas: |
Lastetusmaks, abielu, lapsed olid siis norm.
+ soodustused eluaseme soetamisel, sõltuvuses laste arvust jne. |
Oleme täpsed. Eluaset ei saanud soetada, see eraldati. Aga parema eluaseme ja kiiremini võis saada küll.
Okok, kooperatiivkortrid jms. olid ka, aga nende soetamist ei toetatud kuidagi.
|
|
| Kommentaarid: 79 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
60 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
Tbit
HV Guru
liitunud: 27.04.2004
|
|
15.05.2026 22:33:58
|
|
|
Orbani Ungari ju proovis seda kõike tänapäevases võtmes, ulme raha ja soodustused, tulemus ümmargune null.
Ühelt poolt turg sööb kõik selle vaba raha isuga ära mis antakse, teisalt vaba maailm ja vabad valikud, 20ndad veeta Ibizal möllates või ...
_________________
DVD is da 4483MB :-/)
|OSTAN|-> T43 pikk jahutus |
|
| Kommentaarid: 265 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
3 :: |
230 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
acl
HV vaatleja
liitunud: 02.12.2019
|
|
20.05.2026 09:52:43
|
|
|
Lapsi võib teha nii, et vähe pole, aga kasvatama peab ka neid. Head võluvitsa ei ole olemas, äkki kui, Sul on 3 last, nende töökoormus keerata vähemaks neli päeva nädalas? See enda jaoks aja leidmine on kõige keerulisem, muidugi lapsed kasvades muutuvad iseseisvamaks, aga seni peab kuidagi ka hakkama saama. Pealegi hetkel on see esimese lapse samm see kõige raskem, kui vaadata toetusi, kus esimese lapse kulu on kõige suurem, muidugi lootust on et tuttavatelt saada riideid/mänguasju, aga ega kõike ka ei taha taaskasutatult.
Lisaks veel meedia, kus on rohkem hirmutamist, kui positiivsust. Lisaks on sotsiaalmeedia, mis õpetab kuidagi kavalalt, et saab aru, mis sugu oled ja vastavalt sellele, siis annab sisu, kus näiteks mehe puhul räägitakse, et mida naine valesti teeb suhtes. Naiste puhul tulevad vastupidised videod
No positiivne tegelikult on, et aastamaks alates 7 kohalisest autost on ikka oluliselt odavamaks muudetud.
|
|
| Kommentaarid: 2 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
2 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
Betamax
HV Guru
liitunud: 29.05.2003
|
|
| Kommentaarid: 754 loe/lisa |
Kasutajad arvavad: |
|
:: |
1 :: |
1 :: |
566 |
|
| tagasi üles |
|
|
Taux007
HV veteran

liitunud: 27.08.2005
|
|
21.05.2026 11:00:48
|
|
|
Kuradi nutitelefonid!
Võib vist umbes sinna kanti tõmmata joone ja öelda, et nutitelefonidest hakkas sotsiaalne võõrandumine pihta ja "connecting people" asendus kartusega.
|
|
| Kommentaarid: 47 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
46 |
|
| tagasi üles |
|
|
SKG
HV Ihaldatuim Poissmees

liitunud: 27.01.2003
|
|
21.05.2026 11:31:08
|
|
|
Why birth rates are falling everywhere all at once
Homes and phones are part of the reason for the demographic shift changing our world
https://www.ft.com/content/fba35eca-df3a-4ad6-b42d-eb08eb7c9ad3
Spoiler
The demographic landslide defining our era is gaining speed — and terrain.
In more than two-thirds of the world’s 195 countries, the average number of children born to each woman has fallen below the “replacement rate” of 2.1 that keeps populations stable without immigration. In 66 countries, the average is now closer to one than to two. In some, the most common number of children born to each woman is zero.
Both the pace and the breadth of the decline are defying expectations. Just five years ago the UN predicted there would be 350,000 births in South Korea in 2023. That was a 50 per cent overestimate: the real figure was 230,000.
While high- and middle-income countries have been wrestling with demographic decline for more than half a century, the phenomenon has markedly accelerated in the past 10 years.
Analysis of data ranging from population records to Google searches indicates that although many factors contribute to falling birth rates, the most recent plunge appears connected with our use of technology.
Almost all of the world is now affected. Until recently, ultra-low and rapidly falling birth rates were primarily a concern for rich countries, but many developing countries now have lower fertility rates than much wealthier ones.
In 2023 Mexico’s birth rate fell below that of the US for the first time — as, subsequently, did those of Brazil, Tunisia, Iran and Sri Lanka. Lower- and middle-income countries are now getting old before they get rich.
The defining problem of our time
Population ageing shrinks the workforce and exerts a drag on growth in productivity and living standards — Japan’s stagnation since the 1990s is almost entirely explained by low birth rates that have shrunk its working-age population.
Fiscal pressure from ballooning spending on pensions and care also crowds out investment in infrastructure, helping create a sense of decline that fuels anti-system politics.
“Fertility decline is the big question of our time,” says Jesús Fernández-Villaverde, economics professor at the University of Pennsylvania and a leading researcher on the consequences of demographic change. He argues that almost all pressing problems flow from the collapse in birth rates: “Everything else is downstream.”
One does not have to be Elon Musk, who argues that declining birth rates represent the “biggest risk to civilisation”, to see how they may already be exacerbating many of the world’s social and economic travails.
Some hope a smaller population could help tackle climate change. But a recent study found lower birth rates will have at best a negligible impact on emissions over the coming decades.
Birth rates are often collapsing despite, not because of, people’s desires. Most young men and women still report wanting around two children — even in South Korea where most women now have zero.
Instead, there is a “fertility gap” between goals and outcomes, due to frictions and frustrations that have much to do with modern lifestyles — including our homes and, increasingly, our phones.
Singles’ night forever
In previous decades, the world’s fertility rate went down because couples had fewer children. Now the main reason is that there are fewer couples.
Had US rates of marriage and cohabitation remained constant over the past decade, the country’s total fertility rate would be higher today than it was 10 years ago.
A pioneering study by demographer Stephen Shaw shows that in the US and most high-income countries, the number of children that mothers give birth to is stable or even rising. But the proportion of women who have any children at all has fallen steeply in the past 15 years.
The stereotypes often associated with this trend include women putting careers before children, or couples who choose not to have them despite plenty of disposable income.
But, across a wide range of countries, the decline in births and coupling is much steeper among those with the least education and lowest incomes. By contrast the share of university graduates forming couples and having children is stable or even rising in some cases. Family formation, it seems, has become K-shaped.
Nor has state involvement by rich countries arrested the trend. Since the 1980s, developed countries have tripled real-terms per capita spending on child benefits, subsidised childcare and parental leave while the share of childcare performed by fathers has climbed steadily upwards. Birth rates have declined all the same — from 1.85 to 1.53 per woman.
Many people opt happily for a single life without children. But the data shows that across broader society, the number of people finding partners and having children is declining despite intentions. This is notably pronounced among the least well off, and accompanies mounting loneliness and dating frustrations.
Home economics
In several rich countries, including the US and UK, a major barrier to forming families in recent decades has been housing.
According to FT analysis, as much as half of those countries’ decline in fertility rates since the 1990s can be explained by falling home ownership and a rise in young adults who live with their parents.
In such situations, the absence of long-term housing acts as a barrier to other long-term commitments.
But this cannot account for the most recent steep decline or its global breadth.
In the Nordic region, for example, fertility has fallen despite economic stability and a rise in the number of young adults living on their own, rather than with parents or flatmates.
And even when couples can afford to move into their own place, they are increasingly likely to separate. In several countries, people who move in together are now more likely to split up than to have a child, a sharp reversal of the historical norm.
Other economic factors also fall short of being conclusive.
The recent demographic slide has occurred in countries hard hit by the global financial crisis as well as those virtually unscathed by it, and in both slow-growing western Europe and the rapidly-growing Middle East and south-east Asia.
Many point to young adults’ economic precariousness. But while young people’s earnings peak later than occurred during previous decades and their relative economic standing has declined, these are gradual shifts that do not fit a sudden decline.
Another possible factor is the changing relative positions of young men and women. Girls are now far more likely to attend university than boys, and lower-educated young men are now often out-earned by their female counterparts, changing the calculus for settling down with someone. But these too are mostly slow shifts that apply much more to some parts of the world than others.
The population threat in your pocket
Dissatisfied with purely economic explanations, researchers are beginning to point the finger at a new culprit — the digital devices and platforms that play an outsized role in young people’s lives across the world.
Nathan Hudson and Hernan Moscoso-Boedo of the University of Cincinnati published a paper last month looking at birth rates through the lens of the rollout of 4G mobile networks in the US and UK.
The number of births fell first and fastest in the areas that received high-speed mobile connectivity earliest. The authors argue that smartphones have transformed how young people spend time with one another, sharply reducing in-person socialising and leading to the collapse in their fertility.
FT research indicates the same trend has affected other countries.
For example, US, British and Australian birth rates for teens and young adults were broadly flat during the early 2000s but began to fall markedly from 2007.
The same slide began in France and Poland around 2009, and in Mexico, Morocco and Indonesia around 2012. What had been steady declines in fertility in Ghana, Nigeria and Senegal became precipitous drops between 2013 and 2015.
All of these inflection points coincided with the mass adoption of smartphones in local markets — as measured by Google searches for mobile apps.
US, British and Australian birth rates were relatively stable during the early 2000s but began a marked decline from around 2007
The same slide began in Mexico and Indonesia around 2012
In Iran, Egypt and Senegal, the decline came around 2015
These look like disparate events, but if we shift them to align with the take-off of smartphones in each country...
...and adjust for what was happening to birth rates before phones arrived, we see a unified trend
In country after country the birth rate plunged after the introduction of smartphones, no matter what the previous trend was. The younger the age group, the more pronounced the downturn — a mirror image of smartphone usage patterns.
Melissa Kearney, professor of economics at the University of Notre Dame, says it is “quite plausible that the modern digital media environment has had profound effects on society that have led to a decline in romantic coupling”.
Indeed, Hudson and Moscoso-Boedo’s thesis that the key factor is less time spent socialising in person is supported by evidence from dozens of countries. In South Korea young adult in-person socialising has halved in 20 years.
“To meet a person you are going to marry requires filtering through a lot of people,” says demographer Lyman Stone. “If you socialise much less, it takes you much longer to find a match if you find one at all.”
He adds: “If you spend lots of time socialising with your peers in the real world, your standards [for a potential partner] are anchored in the real world. If you spend your time on Instagram, your standards are anchored to an artificial sense of what is normal.”
Social media leaves its mark
Among couples, sexual dysfunction is higher for the young adults with the heaviest social media use, notes Finnish demographer Anna Rotkirch.
She argues that the time taken up by social media — and the values and lifestyles such platforms project — has also made it harder for young adults to form committed relationships.
Stanford University’s Alice Evans adds that the more traditional a culture is in terms of its gender roles, the greater is the impact of smartphones on birth rates.
The data bears this out: the Middle East and Latin America show many of the steepest birth-rate falls of the past decade, and a recent study found that social media use is associated with lower fertility in Sub-Saharan Africa. In south Asia, where women’s web access is often more limited, fewer people remain single.
Evans describes what she calls “cultural leapfrogging”, adding that “Instagram and TikTok enable young women across the world to bypass traditional authorities . . . raising their expectations for a relationship in a way their male counterparts are often not prepared for”.
FT research has also indicated that the emerging ideological divide between young men and women is a smartphone-era phenomenon, concentrated among the non-college-educated. Among this cohort, women have moved leftward, men have not, and coupling and births have cratered.
One possibility is that social media intensifies and consolidates people’s reactions to trends such as housing difficulties or the changing economic positions of men and women, making decades-long processes feel like sudden waves, amplifying economic concerns, and creating a persistent sense of insecurity and worry that can act as a prophylactic.
Indeed, theories about the impact of new media technologies on relationships and fertility are not new to the smartphone era.
In 2001, researchers Robert Hornik and Emile McAnany found that there was a stronger link between falling birth rates and television ownership than between income or education.
A decade later a study by Eliana La Ferrara and others found that watching TV soap operas that portray small families led women to have fewer children, and in 2018 Adrienne Lucas and Nicholas Wilson found that owning a television led couples to have less sex.
Considering smartphone usage is heavier and more solitary than television viewing, the effects could be much larger.
Time for a solution
What should be done to contend with trends deeply embedded in modern lifestyles?
Governments have to resist the lure of unrealistic solutions — after all, there is no uninventing the smartphone. As Stone says: “If someone has bad eyes, we don’t fix their genes: we give them glasses.”
By contrast, there is ample evidence that providing secure and suitable homes to young couples increases their likelihood of starting a family.
“Baby bonuses” incentivising couples to have children are another option that may arrest the slide — but only if sufficiently generous.
But government resources are limited, economic factors do not alone decide the demographic decline and incentives aimed at helping happy couples to have children may be beside the point when more and more people simply lack partners.
The bigger point is that falling birth rates appear to be part of a broader phenomenon of young adult singledom, isolation and deteriorating wellbeing. Given the likely link to technology and social media, the best hope of reversing the trend may be to change our digital habits — whether through cultural shifts or government regulation.
Even apart from our diminishing propensity to have children, the task of bringing together a fractured and frustrated generation is the challenge of our times.
|
|
| Kommentaarid: 373 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
3 :: |
313 |
|
| tagasi üles |
|
|
netcat
Kreisi kasutaja
liitunud: 13.01.2010
|
|
21.05.2026 13:24:32
|
|
|
Asjalik artikkel 
|
|
| Kommentaarid: 7 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
7 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
Betamax
HV Guru
liitunud: 29.05.2003
|
|
| Kommentaarid: 754 loe/lisa |
Kasutajad arvavad: |
|
:: |
1 :: |
1 :: |
566 |
|
| tagasi üles |
|
|
napoleon
Unknown virus
liitunud: 08.12.2008
|
|
25.05.2026 13:56:30
|
|
|
| Betamax kirjutas: |
| Mida me säilitada tahame? Rahvust või rahvaarvu? |
Teoorias võiks ju mõlemad säilida kui Eesti mehed võtaks naiseks sisserännanu ning Eesti naised meheks samuti sisserännanu ja kasvtakse lastest eestlased.
Praktikas seda ilmselt ei juhtu massiliselt.
|
|
| Kommentaarid: 79 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
60 |
|
| tagasi üles |
|
|
netcat
Kreisi kasutaja
liitunud: 13.01.2010
|
|
25.05.2026 15:27:07
|
|
|
| Tavaliselt kukub see vastupidi välja, või juhtub selline õnnetus nagu meie praeguse haridusministriga. Kes ainult unistab sellest, kuidas saaks eestlastele nende pastlad jätta.
|
|
| Kommentaarid: 7 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
7 |
|
| tagasi üles |
|
|
Hiid
HV Guru
liitunud: 23.03.2002
|
|
25.05.2026 15:56:03
|
|
|
Eesti rahvus on läinud rong, paraku 
_________________
Hapud viinamarjad |
|
| Kommentaarid: 664 loe/lisa |
Kasutajad arvavad: |
|
:: |
3 :: |
0 :: |
512 |
|
| tagasi üles |
|
|
netcat
Kreisi kasutaja
liitunud: 13.01.2010
|
|
25.05.2026 18:19:30
|
|
|
| Väga suure tõenäosusega jah. Aga samas ei tea kunagi, maailma lõpp võib ka enne meie väljasuremist tulla.
|
|
| Kommentaarid: 7 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
7 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
25.05.2026 18:23:26
|
|
|
Loodus tühja kohta ei salli - kui eestlased Eestimaad ei täida, tulevad muud rahvused asemele. Seda lausa soositakse praeguse koalitsiooni poolt.
EDIT: https://forum.fp.lhv.ee/t/reformierakond/27912/5351
| tsitaat: |
Eesti venestamine on Venemaale kasulik tulevikku silmas pidades ja need on puht venelased, Solovjovi ja Kisseljovi auditoorium.
Ma näen seda iga päev isegi Tartus, Tallinna ei taha enam sõitagi, see on juba vene linn rahvastikult
Nüüd tehakse uksed lahti ka Kasahstani jt eks soveti inimestele, kelle jaoks isegi 80 % Eesti keskmisest palgast on meeletu rahasumma, mida nad oma kodumaal kunagi ei näeks.
Miks mitte tulla kui siin on kõikjal vene keel, mida eks-soveti ruumi inimesed ikka oskavad ?
Leedus, Poolas või Soomes nad nii hästi hakkama ei saaks, linnalegend räägib, et Poolas võid venekeelse ülbe jauramise eest tänaval isegi peksa saada. Pika vihaga rahvas, nad ei ole unustanud Katõni jt kuritegusid.
Eestlased on miskipärast unustanud ja küüditaja autahvel ripub senini majaseinal, punasõduri kuju aga mattub lilledesse 9.mail |
_________________
Hinnavaatlus.ee - leia parim hind!
HV-s ID-kaardiga autentimine |
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
Betamax
HV Guru
liitunud: 29.05.2003
|
|
| Kommentaarid: 754 loe/lisa |
Kasutajad arvavad: |
|
:: |
1 :: |
1 :: |
566 |
|
| tagasi üles |
|
|
degrass
HV kasutaja
liitunud: 23.12.2004
|
|
25.05.2026 22:23:18
|
|
|
RE ja E200 süüdistamine kõigis surmapattudes on suunatud rumalatele. Klassikaline sisevaenlase narratiiv.
Iibe teema on niivõrd kompleksne, peab väga rumal olema, arvamaks, et on olemas lihtsaid lahendusi. Stiilinätena võib mainida paari aasta eest mingite vanameeste soovi naisi lastetuse teemal küsitleda. Muidugi on neil mugav naisi süüdistada, sest nemad käisid ülikoolis ja tegid karjääri.
PS. Kui tööandja plaanib 10% töötajaid aasta jooskul välja vahetada on see kindlasti perekonna planeerimisel abiks.
_________________
All it took was for a lot of seemingly decent people to put the wrong person in power, and then pay for their innocent choice. |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
25.05.2026 22:37:45
|
|
|
Immigratsiooni hoogustamisega praegune koalitsioon ei pea Eesti Põhiseadust ega eestlaste ellujäämisvõimet millekski.
P.S. Selle küsitluse mõte oli siiras - teada saada, miks noored lapsi enam ei taha.
Aga selle vastuse teadasaamiseks pole vaja isegi enam küsitlust korraldada.
_________________
Hinnavaatlus.ee - leia parim hind!
HV-s ID-kaardiga autentimine |
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
degrass
HV kasutaja
liitunud: 23.12.2004
|
|
25.05.2026 22:58:35
|
|
|
Tanel, vastasin sinu küsimusele eespool.
_________________
All it took was for a lot of seemingly decent people to put the wrong person in power, and then pay for their innocent choice. |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
Taux007
HV veteran
liitunud: 27.08.2005
|
|
26.05.2026 12:40:49
|
|
|
| Küsitluse tulemusi vaadates pole ka ime, et 30+ saadakse esimene laps. Rahval pole huvi ja viitsimist jännata lastega.
|
|
| Kommentaarid: 47 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
46 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
bugbrake
HV kasutaja
liitunud: 10.12.2006
|
|
28.05.2026 10:59:39
|
|
|
| SKG kirjutas: |
Why birth rates are falling everywhere all at once
Homes and phones are part of the reason for the demographic shift changing our world
https://www.ft.com/content/fba35eca-df3a-4ad6-b42d-eb08eb7c9ad3
Spoiler
The demographic landslide defining our era is gaining speed — and terrain.
In more than two-thirds of the world’s 195 countries, the average number of children born to each woman has fallen below the “replacement rate” of 2.1 that keeps populations stable without immigration. In 66 countries, the average is now closer to one than to two. In some, the most common number of children born to each woman is zero.
Both the pace and the breadth of the decline are defying expectations. Just five years ago the UN predicted there would be 350,000 births in South Korea in 2023. That was a 50 per cent overestimate: the real figure was 230,000.
While high- and middle-income countries have been wrestling with demographic decline for more than half a century, the phenomenon has markedly accelerated in the past 10 years.
Analysis of data ranging from population records to Google searches indicates that although many factors contribute to falling birth rates, the most recent plunge appears connected with our use of technology.
Almost all of the world is now affected. Until recently, ultra-low and rapidly falling birth rates were primarily a concern for rich countries, but many developing countries now have lower fertility rates than much wealthier ones.
In 2023 Mexico’s birth rate fell below that of the US for the first time — as, subsequently, did those of Brazil, Tunisia, Iran and Sri Lanka. Lower- and middle-income countries are now getting old before they get rich.
The defining problem of our time
Population ageing shrinks the workforce and exerts a drag on growth in productivity and living standards — Japan’s stagnation since the 1990s is almost entirely explained by low birth rates that have shrunk its working-age population.
Fiscal pressure from ballooning spending on pensions and care also crowds out investment in infrastructure, helping create a sense of decline that fuels anti-system politics.
“Fertility decline is the big question of our time,” says Jesús Fernández-Villaverde, economics professor at the University of Pennsylvania and a leading researcher on the consequences of demographic change. He argues that almost all pressing problems flow from the collapse in birth rates: “Everything else is downstream.”
One does not have to be Elon Musk, who argues that declining birth rates represent the “biggest risk to civilisation”, to see how they may already be exacerbating many of the world’s social and economic travails.
Some hope a smaller population could help tackle climate change. But a recent study found lower birth rates will have at best a negligible impact on emissions over the coming decades.
Birth rates are often collapsing despite, not because of, people’s desires. Most young men and women still report wanting around two children — even in South Korea where most women now have zero.
Instead, there is a “fertility gap” between goals and outcomes, due to frictions and frustrations that have much to do with modern lifestyles — including our homes and, increasingly, our phones.
Singles’ night forever
In previous decades, the world’s fertility rate went down because couples had fewer children. Now the main reason is that there are fewer couples.
Had US rates of marriage and cohabitation remained constant over the past decade, the country’s total fertility rate would be higher today than it was 10 years ago.
A pioneering study by demographer Stephen Shaw shows that in the US and most high-income countries, the number of children that mothers give birth to is stable or even rising. But the proportion of women who have any children at all has fallen steeply in the past 15 years.
The stereotypes often associated with this trend include women putting careers before children, or couples who choose not to have them despite plenty of disposable income.
But, across a wide range of countries, the decline in births and coupling is much steeper among those with the least education and lowest incomes. By contrast the share of university graduates forming couples and having children is stable or even rising in some cases. Family formation, it seems, has become K-shaped.
Nor has state involvement by rich countries arrested the trend. Since the 1980s, developed countries have tripled real-terms per capita spending on child benefits, subsidised childcare and parental leave while the share of childcare performed by fathers has climbed steadily upwards. Birth rates have declined all the same — from 1.85 to 1.53 per woman.
Many people opt happily for a single life without children. But the data shows that across broader society, the number of people finding partners and having children is declining despite intentions. This is notably pronounced among the least well off, and accompanies mounting loneliness and dating frustrations.
Home economics
In several rich countries, including the US and UK, a major barrier to forming families in recent decades has been housing.
According to FT analysis, as much as half of those countries’ decline in fertility rates since the 1990s can be explained by falling home ownership and a rise in young adults who live with their parents.
In such situations, the absence of long-term housing acts as a barrier to other long-term commitments.
But this cannot account for the most recent steep decline or its global breadth.
In the Nordic region, for example, fertility has fallen despite economic stability and a rise in the number of young adults living on their own, rather than with parents or flatmates.
And even when couples can afford to move into their own place, they are increasingly likely to separate. In several countries, people who move in together are now more likely to split up than to have a child, a sharp reversal of the historical norm.
Other economic factors also fall short of being conclusive.
The recent demographic slide has occurred in countries hard hit by the global financial crisis as well as those virtually unscathed by it, and in both slow-growing western Europe and the rapidly-growing Middle East and south-east Asia.
Many point to young adults’ economic precariousness. But while young people’s earnings peak later than occurred during previous decades and their relative economic standing has declined, these are gradual shifts that do not fit a sudden decline.
Another possible factor is the changing relative positions of young men and women. Girls are now far more likely to attend university than boys, and lower-educated young men are now often out-earned by their female counterparts, changing the calculus for settling down with someone. But these too are mostly slow shifts that apply much more to some parts of the world than others.
The population threat in your pocket
Dissatisfied with purely economic explanations, researchers are beginning to point the finger at a new culprit — the digital devices and platforms that play an outsized role in young people’s lives across the world.
Nathan Hudson and Hernan Moscoso-Boedo of the University of Cincinnati published a paper last month looking at birth rates through the lens of the rollout of 4G mobile networks in the US and UK.
The number of births fell first and fastest in the areas that received high-speed mobile connectivity earliest. The authors argue that smartphones have transformed how young people spend time with one another, sharply reducing in-person socialising and leading to the collapse in their fertility.
FT research indicates the same trend has affected other countries.
For example, US, British and Australian birth rates for teens and young adults were broadly flat during the early 2000s but began to fall markedly from 2007.
The same slide began in France and Poland around 2009, and in Mexico, Morocco and Indonesia around 2012. What had been steady declines in fertility in Ghana, Nigeria and Senegal became precipitous drops between 2013 and 2015.
All of these inflection points coincided with the mass adoption of smartphones in local markets — as measured by Google searches for mobile apps.
US, British and Australian birth rates were relatively stable during the early 2000s but began a marked decline from around 2007
The same slide began in Mexico and Indonesia around 2012
In Iran, Egypt and Senegal, the decline came around 2015
These look like disparate events, but if we shift them to align with the take-off of smartphones in each country...
...and adjust for what was happening to birth rates before phones arrived, we see a unified trend
In country after country the birth rate plunged after the introduction of smartphones, no matter what the previous trend was. The younger the age group, the more pronounced the downturn — a mirror image of smartphone usage patterns.
Melissa Kearney, professor of economics at the University of Notre Dame, says it is “quite plausible that the modern digital media environment has had profound effects on society that have led to a decline in romantic coupling”.
Indeed, Hudson and Moscoso-Boedo’s thesis that the key factor is less time spent socialising in person is supported by evidence from dozens of countries. In South Korea young adult in-person socialising has halved in 20 years.
“To meet a person you are going to marry requires filtering through a lot of people,” says demographer Lyman Stone. “If you socialise much less, it takes you much longer to find a match if you find one at all.”
He adds: “If you spend lots of time socialising with your peers in the real world, your standards [for a potential partner] are anchored in the real world. If you spend your time on Instagram, your standards are anchored to an artificial sense of what is normal.”
Social media leaves its mark
Among couples, sexual dysfunction is higher for the young adults with the heaviest social media use, notes Finnish demographer Anna Rotkirch.
She argues that the time taken up by social media — and the values and lifestyles such platforms project — has also made it harder for young adults to form committed relationships.
Stanford University’s Alice Evans adds that the more traditional a culture is in terms of its gender roles, the greater is the impact of smartphones on birth rates.
The data bears this out: the Middle East and Latin America show many of the steepest birth-rate falls of the past decade, and a recent study found that social media use is associated with lower fertility in Sub-Saharan Africa. In south Asia, where women’s web access is often more limited, fewer people remain single.
Evans describes what she calls “cultural leapfrogging”, adding that “Instagram and TikTok enable young women across the world to bypass traditional authorities . . . raising their expectations for a relationship in a way their male counterparts are often not prepared for”.
FT research has also indicated that the emerging ideological divide between young men and women is a smartphone-era phenomenon, concentrated among the non-college-educated. Among this cohort, women have moved leftward, men have not, and coupling and births have cratered.
One possibility is that social media intensifies and consolidates people’s reactions to trends such as housing difficulties or the changing economic positions of men and women, making decades-long processes feel like sudden waves, amplifying economic concerns, and creating a persistent sense of insecurity and worry that can act as a prophylactic.
Indeed, theories about the impact of new media technologies on relationships and fertility are not new to the smartphone era.
In 2001, researchers Robert Hornik and Emile McAnany found that there was a stronger link between falling birth rates and television ownership than between income or education.
A decade later a study by Eliana La Ferrara and others found that watching TV soap operas that portray small families led women to have fewer children, and in 2018 Adrienne Lucas and Nicholas Wilson found that owning a television led couples to have less sex.
Considering smartphone usage is heavier and more solitary than television viewing, the effects could be much larger.
Time for a solution
What should be done to contend with trends deeply embedded in modern lifestyles?
Governments have to resist the lure of unrealistic solutions — after all, there is no uninventing the smartphone. As Stone says: “If someone has bad eyes, we don’t fix their genes: we give them glasses.”
By contrast, there is ample evidence that providing secure and suitable homes to young couples increases their likelihood of starting a family.
“Baby bonuses” incentivising couples to have children are another option that may arrest the slide — but only if sufficiently generous.
But government resources are limited, economic factors do not alone decide the demographic decline and incentives aimed at helping happy couples to have children may be beside the point when more and more people simply lack partners.
The bigger point is that falling birth rates appear to be part of a broader phenomenon of young adult singledom, isolation and deteriorating wellbeing. Given the likely link to technology and social media, the best hope of reversing the trend may be to change our digital habits — whether through cultural shifts or government regulation.
Even apart from our diminishing propensity to have children, the task of bringing together a fractured and frustrated generation is the challenge of our times.
|
Tõesti hea artikkel.
Tanel võiks selle ka läbi lugeda. Väga lihtne ja kitsas maailmavaateline lähenemine kui selle süüdistada ainult Reformi ja E200, oleks siis asjad nii lihtsad.
Vaata seda näitajat läbi ajaloo. '80 ja selle lõpp oli see positiivne, peale taasiseseisvumist jälle kõvasti negatiivne jne. Lääne arenenud heaolu- ja tööstusriikide seas ei ole tänapäeval vist ühtegi riiki, kus sündimuskordaja oleks üle 2,1. See probleem laiem ja sügavam. Ma mõistan su viha Reformi ja E200 vastu aga no nii mõjuvõimsad tegijad nad ka pole. Isegi kui Isamaa saaks järgmiseks 10 aastaks ainuvmõmu siis kahtlen kõvasti kas nad suudaks seda numbrit positiivseni viia.
Sellele probleemile võiks ja peaks lähenema täiesti apoliitiliselt ja erakonna üleselt (nii nagu sõjalisse kaitsesse).
_________________
Alati teadke, et kuulujutte mõtlevad välja vihkajad, levitavad lollid, aga usuvad idioodid. |
|
| Kommentaarid: 6 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
6 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
napoleon
Unknown virus
liitunud: 08.12.2008
|
|
30.05.2026 11:03:16
|
|
|
Lõpetuseks tõdeb ka autor, et ega mingit võluvitsa ei ole.
Aga titavabrik on pisut kummaline idee isegi kui meil oleks tehniline võimekus see ehitada. Palju neid naisi ikka on, kes ise sünnitada ei taha, aga kui vabrikust saaks tita tellida, siis oleks nõus ta üles kasvatama. Ok, mingi kogus neid muidugi on, kes laste saamist edasi lükkavad seniks kuni ei ole enam võimelised neid ise saama.
|
|
| Kommentaarid: 79 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
60 |
|
| tagasi üles |
|
|
Ricki
HV kasutaja
liitunud: 02.03.2003
|
|
30.05.2026 11:40:32
|
|
|
| tsitaat: |
mingi kogus neid muidugi on, kes laste saamist edasi lükkavad seniks kuni ei ole enam võimelised neid ise saama.
|
https://novaator.err.ee/1609097786/eesti-inimesed-saavad-lapsi-uha-enam-peale-parim-enne-moodumist
| tsitaat: |
Kui maailma vanim esmasünnitaja oli 73-aastaselt lapse saanud Erramatti Mangamma, siis Kase sõnul Eestist nii äärmuslikke näiteid ei leia. Küll aga sünnitas 2022. aastal tervise arengu instituudi andmetel viis naist esimest korda vähemalt 50-aastaselt. Kõik need naised jäid rasedaks kunstliku viljastamise teel.
"Eesti seadus on selline, et saame kunstlikku viljastamist teha kuni 50-aastasele naisele, hiljem mitte. Samas igas riigis on erinevad seadused. Mõnes riigis ei ole ülempiiri üldse. Siis tõesti saab teha ka 70- või 80-aastasele naisele kunstlikku viljastamist," võrdles naistearst. Sestap on ka Eesti vanim esmasünnitaja olnud 51-aastane.
Kase sõnul näeb ta andmeid vaadates, et üha enam naisi sünnitab Eestis esimest korda enam kui 35-aastastelt. Alla 24-aastaste sünnitajate arv samas väheneb. "Eelmise aasta andmetel oli küll kõige suurem sünnitajate arv vanuserühmas 30–34, aga üldisest statistikast näeme, et aasta-aastalt just see 35+ rühm suureneb," osutas ta. |
https://www.postimees.ee/1455253/66-aastane-naine-sunnitas-tutre
|
|
| Kommentaarid: 3 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
3 |
|
| tagasi üles |
|
|
commer
HV Guru

liitunud: 03.10.2002
|
|
| Kommentaarid: 930 loe/lisa |
Kasutajad arvavad: |
|
:: |
3 :: |
2 :: |
715 |
|
| tagasi üles |
|
|
netcat
Kreisi kasutaja
liitunud: 13.01.2010
|
|
08.06.2026 13:54:12
|
|
|
| Siis sisuliselt võid sa seda asja vaadata nii, et pead 2 lapse lasteaia eest maksma ise ainult 20, ülejäänu saad maksta toetuse eest, abiks seegi vaesel ajal või mis?
|
|
| Kommentaarid: 7 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
7 |
|
| tagasi üles |
|
|
greaper
HV kasutaja

liitunud: 27.06.2005
|
|
09.06.2026 08:38:54
|
|
|
| tsitaat: |
2 lapse toetus 160.-
2 lapse lasteaia arved 180.-
|
See toetus ju ei ole midagi muud, kui poliitiku poolne hääle ostmine sinu enda (maksumaksja) rahaga  , kohatasu on 90, ehk annad 80 toetust kohe tagasi ja maksad veel 10 peale ka , kohatasu on 90, ehk annad 80 toetust kohe tagasi ja maksad veel 10 peale ka
Igasugused riigipoolsed "toetused" on juba teenuste jms hinda sisse arvestatud, päris kindlalt oleks hinnad paremad, kui toetuseid ei oleks (ehe näide igast kaskod jms kus kindlustuse rahaga läheb lihtne remont ulmelise hinnaga, kerge kõks ringil, vanem auto, kõrvalistuja poolne uks mõlkis, kindlustusele esitati arve 4500 ).
_________________
Psychologists usually attribute belief in conspiracy theories to a number of psychopathological conditions such as paranoia, schizotypy, narcissism, and insecure attachment, or to a form of cognitive bias called "illusory pattern perception". |
|
| Kommentaarid: 25 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
24 |
|
| tagasi üles |
|
|
netcat
Kreisi kasutaja
liitunud: 13.01.2010
|
|
| Kommentaarid: 7 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
7 |
|
| tagasi üles |
|
|
Taux007
HV veteran
liitunud: 27.08.2005
|
|
10.06.2026 06:32:07
|
|
|
| greaper kirjutas: |
| tsitaat: |
2 lapse toetus 160.-
2 lapse lasteaia arved 180.-
|
See toetus ju ei ole midagi muud, kui poliitiku poolne hääle ostmine sinu enda (maksumaksja) rahaga , kohatasu on 90, ehk annad 80 toetust kohe tagasi ja maksad veel 10 peale ka
Igasugused riigipoolsed "toetused" on juba teenuste jms hinda sisse arvestatud, päris kindlalt oleks hinnad paremad, kui toetuseid ei oleks (ehe näide igast kaskod jms kus kindlustuse rahaga läheb lihtne remont ulmelise hinnaga, kerge kõks ringil, vanem auto, kõrvalistuja poolne uks mõlkis, kindlustusele esitati arve 4500 ). |
Kas sa reaalselt ka arvad, et 80€ lasteaiakoha eest kuus maksta on selle teenuse reaalne hind?
|
|
| Kommentaarid: 47 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
46 |
|
| tagasi üles |
|
|
greaper
HV kasutaja
liitunud: 27.06.2005
|
|
10.06.2026 08:19:44
|
|
|
| tsitaat: |
Kas sa reaalselt ka arvad, et 80€ lasteaiakoha eest kuus maksta on selle teenuse reaalne hind?
|
Kust sa selle välja lugesid? Jutt käis lapsevanema omaosalusest, mitte selelst palju tegelikult see koht riigile/omavalitsusele (maksumaksjale) maksab. Jutu mõte, igasugused toetused kirjutatakse väga tihti kohe teenuse/toote hinda sisse, sest pakkuja näeb, et "kliendi" maksevõime ju kasvas ja ilma toetuseta oleks mõned teenused/tooted odavamad kliendile (vähemalt päris turumajanduses)
_________________
Psychologists usually attribute belief in conspiracy theories to a number of psychopathological conditions such as paranoia, schizotypy, narcissism, and insecure attachment, or to a form of cognitive bias called "illusory pattern perception". |
|
| Kommentaarid: 25 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
24 |
|
| tagasi üles |
|
|
Taux007
HV veteran
liitunud: 27.08.2005
|
|
10.06.2026 09:08:17
|
|
|
| Suures plaanis nõustun aga lasteaiakoha omahinnastamine küll sellesse loogikasse ei mahu. Võtsin suvaliselt lahti Viljandi valla määruse kohatasu osas ja seal on 25€. Tallinnas on see 50€, Rae vallas 120€. Lastetoetus on kõigis kolmes kohas ühesugune.
|
|
| Kommentaarid: 47 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
46 |
|
| tagasi üles |
|
|
netcat
Kreisi kasutaja
liitunud: 13.01.2010
|
|
18.06.2026 12:54:32
|
|
|
Lihtsaid lahendusi ei ole (kui neid üldse on), kuid see-eest on lihtsad põhjused.
https://teadus.postimees.ee/8493461/usast-leiti-pohjus-miks-seal-on-sundimus-langusse-lainud-sama-asjaolu-voib-mojutada-ka-eestit-ja-muudki-maailma
| tsitaat: |
Majandusteadlased Caitlin Myers ja Ezekiel Hooper jõuavad järeldusele, et nutitelefonide levik võis selgitada koguni kolmandiku kuni poole USA sündimuse langusest aastatel 2007–2011. Nende hinnangul ei ole tegemist lihtsalt juhusliku kokkulangevusega, vaid suure ühiskondliku muutusega, mis muutis inimeste suhtlemist, seksuaalkäitumist ja lõpuks ka laste saamist.
|
| tsitaat: |
Kui 2007. aastal sündis 1000 fertiilses eas naise kohta ligikaudu 70 last, siis 2024. aastaks oli see näitaja langenud 54-ni – umbes 22 protsenti vähem.
Pikka aega peeti peamiseks süüdlaseks 2008. aasta majanduskriisi. Sündimus kipub majanduse halvenedes langema ja paranedes taastuma. Kuid seekord seda ei juhtunud. Sündimus jätkas vähenemist ka järgneval majanduskasvu perioodil. Langus puudutas peaaegu kõiki elanikkonnarühmi sõltumata haridusest, rassist või perekonnaseisust.
|
| tsitaat: |
Teadlaste arvates peab iga tõsiseltvõetav seletus vastama kolmele tingimusele. Mõju peab olema suur, muutus peab algama umbes 2007. aastal ning see peab mõjutama väga laia elanikkonnarühma. Nutitelefonid vastavad kõigile kolmele tingimusele.
|
| tsitaat: |
Maakondades, kus iPhone jõudis inimesteni kiiremini, vähenes sündimus oluliselt rohkem kui piirkondades, kus selle kasutamine oli piiratud. Kõige suurem mõju ilmnes noorte seas. 15–19-aastaste sünnitajate arv vähenes hinnanguliselt 4,5–8 protsenti ning 20–24-aastaste seas 3,2–6,6 protsenti. Vanemates vanuserühmades oli mõju väiksem, kuid siiski sageli siiski statistiliselt oluline.
|
| tsitaat: |
Üldiselt hindavad autorid, et iPhone'i levik põhjustas 33–52 protsenti kogu USA sündimuse vähenemisest aastatel 2007–2011. Teisisõnu võib ligi pool sündimuse langusest olla seotud ühe tehnoloogilise uuendusega.
|
|
|
| Kommentaarid: 7 loe/lisa |
Kasutajad arvavad: |
|
:: |
0 :: |
0 :: |
7 |
|
| tagasi üles |
|
|
Tanel
HV Guru
liitunud: 01.10.2001
|
|
| Kommentaarid: 465 loe/lisa |
Kasutajad arvavad: |
|
:: |
5 :: |
7 :: |
362 |
|
| tagasi üles |
|
|
|
| lisa lemmikuks |
|
 |
sa ei või postitada uusi teemasid siia foorumisse
sa ei või vastata selle foorumi teemadele
sa ei või muuta oma postitusi selles foorumis
sa ei või kustutada oma postitusi selles foorumis
sa ei või vastata küsitlustele selles foorumis
sa ei saa lisada manuseid selles foorumis
sa võid manuseid alla laadida selles foorumis
|
|
Hinnavaatlus ei vastuta foorumis tehtud postituste eest.
|